
In April 2020, the U.S. Centers for Disease Control issued a report featuring evidence that in the month of March 2020, the coronavirus pandemic was not an equal-opportunity killer. Within just a couple of months of COVID-19 emerging in America, it became clear that health disparities were evident in outcomes due to complications from the coronavirus.
 An update from that early look at differences in COVID-19 diagnoses and mortality rates was published in Health Disparities by Race and Ethnicity During the COVID-19 Pandemic: Current Evidence and Policy Approaches, In this report, the Assistant Secretary for Planning and Evaluation, part of the Department of Health and Human Services, provides the evidence on health disparities and social determinants by race and ethnicity through March 10, 2021 starting from January 21, 2020 considered the start of the pandemic in the United States.
An update from that early look at differences in COVID-19 diagnoses and mortality rates was published in Health Disparities by Race and Ethnicity During the COVID-19 Pandemic: Current Evidence and Policy Approaches, In this report, the Assistant Secretary for Planning and Evaluation, part of the Department of Health and Human Services, provides the evidence on health disparities and social determinants by race and ethnicity through March 10, 2021 starting from January 21, 2020 considered the start of the pandemic in the United States.
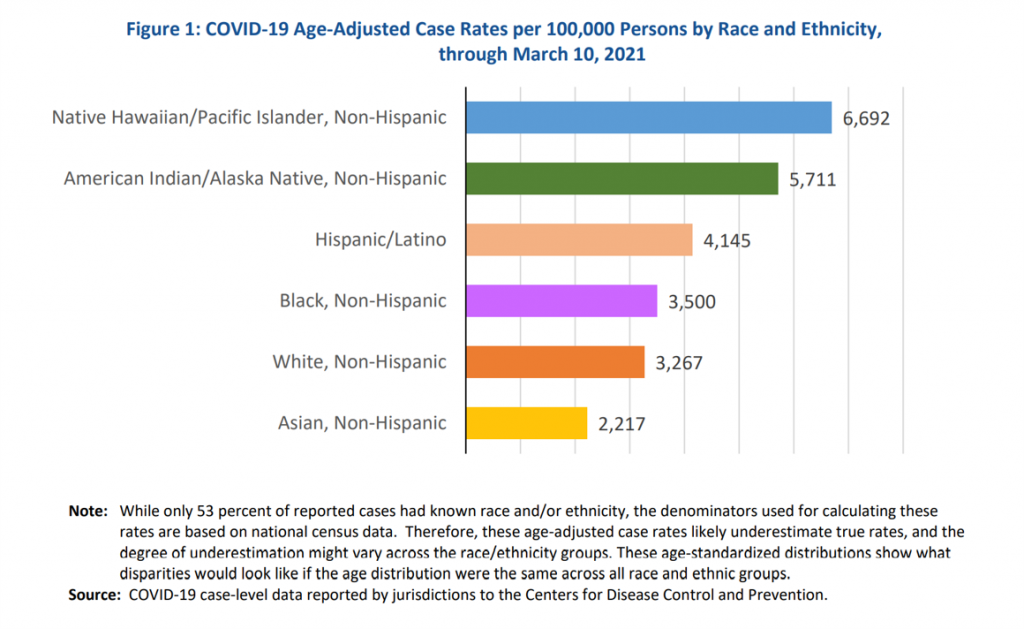
In the U.S., people who are part of Native and Pacific Islander, American Indian and Alaska Native, Hispanic and Latinx, and Black (non-Hispanic) communities were more likely to have had a COVID-19 diagnosis in the first fourteen months of the pandemic than people were White or Asian citizens.
Note that the case rate per 100,000 for White, non-Hispanic people in the U.S. was half that for Native Hawaiian/Pacific Islanders. The first chart summarizes the COVID-19 case rates per 100,000 people by race and ethnicity, 74% greater for American Indian/Alaska Native people, 27% greater for Hispanic and Latinx folks, and about 7% greater for Black people.
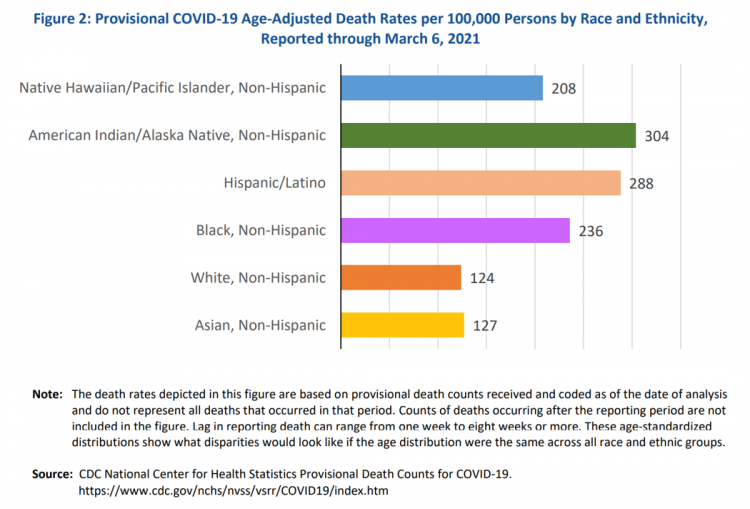
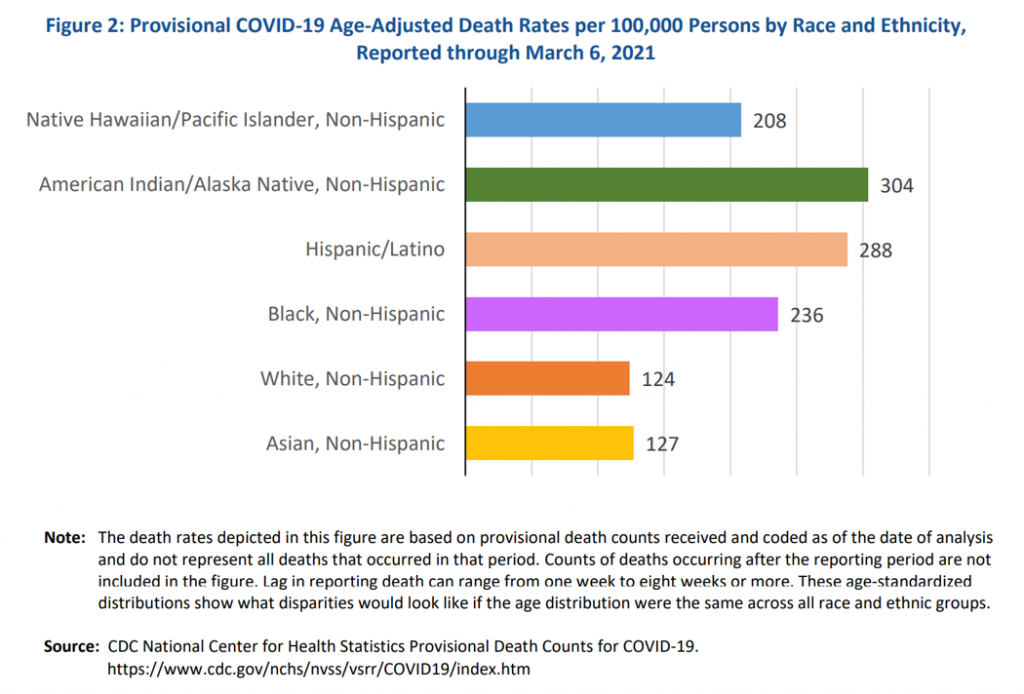 When it comes to death rates, Black people in the U.S. had a much greater risk or mortality due to COVID-19 than Whites in the first fourteen months of the pandemic; Black people in America were nearly twice as likely as white people to die due to the coronavirus, the second chart starkly illustrates (124 deaths per 100,000 for whites versus 236 deaths per 100,000 for Blacks).
When it comes to death rates, Black people in the U.S. had a much greater risk or mortality due to COVID-19 than Whites in the first fourteen months of the pandemic; Black people in America were nearly twice as likely as white people to die due to the coronavirus, the second chart starkly illustrates (124 deaths per 100,000 for whites versus 236 deaths per 100,000 for Blacks).
Other people of color were much more likely to be at-risk for death due to COVID-19 than White Americans, except for Asian people who were on-par for death due to C19 with White people, the chart shows.
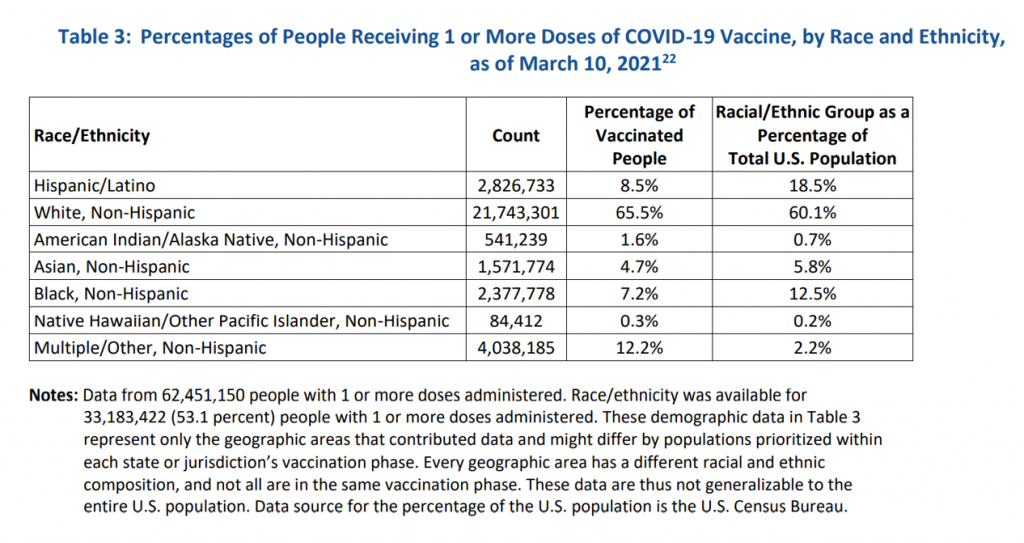
The rate of vaccinations against the coronavirus, too, significantly varied by race and ethnicity as of March 11, 2021. ASPE analyzed data from 62,451,150 people who had 1 or more vaccine doses administered by 3-10-21.
The percentages of people in the U.S. who had received 1 or more doses of COVID-19 vaccines by race/ethnicity were:
- 66% of White, non-Hispanic people (60% of U.S. population)
- 8.5% of Hispanic and LatinX people (19% of U.S. population)
- 7.2% of Black, non-Hispanic people (13% of U.S> population)
- 4.7% of Asian people (6% of U.S. population)
- 1.6% of American Indian/Alaska Native people (less than 1% of U.S. population)
- 0.3% of Native Hawaiian/Other Pacific Islander people (0.2% of U.S. population).
 There are several factors underlying these statistics of health and healthcare inequities. ASPE points to, “long-standing systemic inequalities and structural racism” at the start of the Agency’s discussion of the disparities. Analyzing county-level data for 3,142 U.S. counties revealed that most of observed racial disparities for COVID-19 deaths persisted after controlling for overall 2019 mortality rates and COVID-19 cases per 100,000. suggested social determinants were at play in the disparate outcomes for people of color.
There are several factors underlying these statistics of health and healthcare inequities. ASPE points to, “long-standing systemic inequalities and structural racism” at the start of the Agency’s discussion of the disparities. Analyzing county-level data for 3,142 U.S. counties revealed that most of observed racial disparities for COVID-19 deaths persisted after controlling for overall 2019 mortality rates and COVID-19 cases per 100,000. suggested social determinants were at play in the disparate outcomes for people of color.
For some people such as American Indian and Native Alaskan folks, geography, remoteness, and lack of public health infrastructure are challenges. For people who are Black and Hispanic, lack of high school degrees, and greater density of people living in homes can contribute to poor outcomes from the coronavirus due to spread or access to resources like broadband or health care insurance (which some working people lost due to job loss, furlough, or cut hours in the pandemic). It has also recently been found that language barriers have contributed to poor health outcomes, making the case for linguistically tailored services and community-health workers who are based in peoples’ neighborhoods.
To address these differences, ASPE offers several recommendations including improving public health data infrastructure-collection-dissemination to inform evidence-based decisions, considering the intersection of people of color and disabilities/chronic conditions, ensuring equitable access to critical COVID-19 equipment and supplies, and expanding access to health care and social services especially for language and literacy, mental health services, community and home-based services, and telehealth. In addition, policies that address underlying social determinant risk factors like housing, jobs, food security, and access to social services would be critical, ASPE believes.
Health Populi’s Hot Points: In the pandemic, millions of people who felt symptoms of COVID-19 avoided seeking care due to cost and/or access challenges (of which cost is a key factor). In the public health crisis, retail pharmacies and grocery stores with embedded pharmacies played major roles in providing counsel, primary care, and of course the core business of channeling medicines across the counter. Pharmacists continue to enjoy high levels of trust among U.S. adults, the annual Gallup survey on honesty and ethics in professions perennially proves.
An interesting model to consider of a pharmacy taking on a role in bolstering social determinants for good health is a venture announced this week between AllianceRx Walgreens Prime and Highmark: a specialty pharmacy and a health insurance organization. In this pilot, Walgreens’ specialty pharmacy AllianceRx Walgreens Prime is collaborating with Highmark Blue Cross and Blue Shield plan to address social determinants risks in a patient population dealing with multiple sclerosis (MS).
The program will identify MS patients at risk of SDoHs to be able to make referrals for services such as mental and behavioral health, social work, food security, and other challenges facing people dealing with MS.
“The outreach conducted through this pilot program is the first step to help ensure members who are already facing health challenges have the support and resources they need to overcome barriers in other aspects of their lives which impact their health,” Amy Shannon, director of health and well-being integration at Highmark, stated in the program’s press release.
 The program will deploy nurses trained in the field of social determinants of health from the AllianceRx Walgreens Prime network, who will reach out to Highmark members that opt-in to the pilot. The nurses will conduct a 13-question SDoH survey and assess risk factors that compromise the good management of patients’ MS conditions. “Expanding assessment capabilities to include SDoH factors is a natural progression in the role of a specialty pharmacy,” Rick Miller, VP of clinical and professional services at AllianceRx Walgreens Prime believes.
The program will deploy nurses trained in the field of social determinants of health from the AllianceRx Walgreens Prime network, who will reach out to Highmark members that opt-in to the pilot. The nurses will conduct a 13-question SDoH survey and assess risk factors that compromise the good management of patients’ MS conditions. “Expanding assessment capabilities to include SDoH factors is a natural progression in the role of a specialty pharmacy,” Rick Miller, VP of clinical and professional services at AllianceRx Walgreens Prime believes.
Highmark, which covers health insurance for members in Delaware, New York, Pennsylvania, and West Virginia, has been working on social determinants of health programs for several years. In April 2020, in the early phase of COVID-19, Highmark launched a digital referral tool called “Aunt Bertha” to connect people to services in its target markets and nationally. Providers serving Highmark members can use the referral tool for people who need access to social/health services such as food, housing, transportation, and mental health support.
Returning to the ASPE report on health disparities due to COVID-19, we re-state the recommendation that, “Policies that address underlying social determinant risk factors like housing, jobs, food security, and access to social services would be critical.”
In the U.S., the private sector has been stepping in to fill some of the social determinants gaps and address risks of food in-security, transportation inaccessibility, and housing (for example, programs from UnitedHealthcare and Kaiser Permanente have been addressing the challenge of housing access for their communities). These are in fact infrastructure and social/health care factors that are nationally scalable with public policy and funding. We look forward to seeing some of these factors bundled into infrastructure policy in the coming months which can help address the health inequities long plaguing U.S. health care, exacerbated by COVID-19.

